






There’s one statistic that drops the mic every time: 75% of new clients drop out of behavioral healthcare before their third appointment.
That’s not just before treatment ends. That’s before it even gets started.
That stat came from Scott Lloyd, President of MTM Consulting Services, during a recent National Council-hosted webinar on premature dropout.
Scott was joined by Eleos CCO Dennis Morrison, PhD for the webinar, titled, From First Appointment to Third Visit: Strategies to Reduce Premature Dropout. ICYMI: Watch the on-demand recording here!
It turns out Scott was full of mind-blowing stats—and the one above wasn’t the only one that stings. Client tenure (the average number of visits a client actually attends) has dropped 86.7% from pre-COVID levels. The modal number of sessions in the industry—the most common number—is one.
If we’re honest about what that means, it means a lot of people are walking through the door and never coming back. And the reasons are more preventable than most organizations want to admit. But that’s why you’re here.
The Access Gap We’re Not Measuring
Before we can even really talk about premature dropout, we have to talk about what access actually means.
One of the first things Scott unpacked was the difference between how organizations define “access” and how clients experience it. Organizations tend to measure wait time to the assessment appointment and call it done. But in reality, clients experience two wait times—the wait before the first appointment, and the wait for the next one, a pile of paperwork, and then, if they make it that far, a treatment plan built on 90 minutes of knowing them.
Nationally, the average time from a client’s first call to actually arriving for care is 48 days. For therapy-only (no psych eval), it’s 31 days. SAMHSA and the CCBHC framework have started tracking “time to third appointment” precisely because regulators noticed that shortening wait time one just pushed the problem to wait time two.
“When a consumer calls for help,” Scott explained, “they look at wait time number one. And for 99% of the organizations that we work with, at that point, they’re checking the box. The time clock stops, and they say, ‘Hey, now they’re in, we can bill for them.'” But the client’s experience doesn’t end there, because they’re still waiting to get into actual care.
Why the First Session Is Working Against You
Denny Morrison, PhD, Chief Clinical Officer at Eleos, brought the clinical research perspective, reframing the dropout problem in a way that’s hard to unsee.
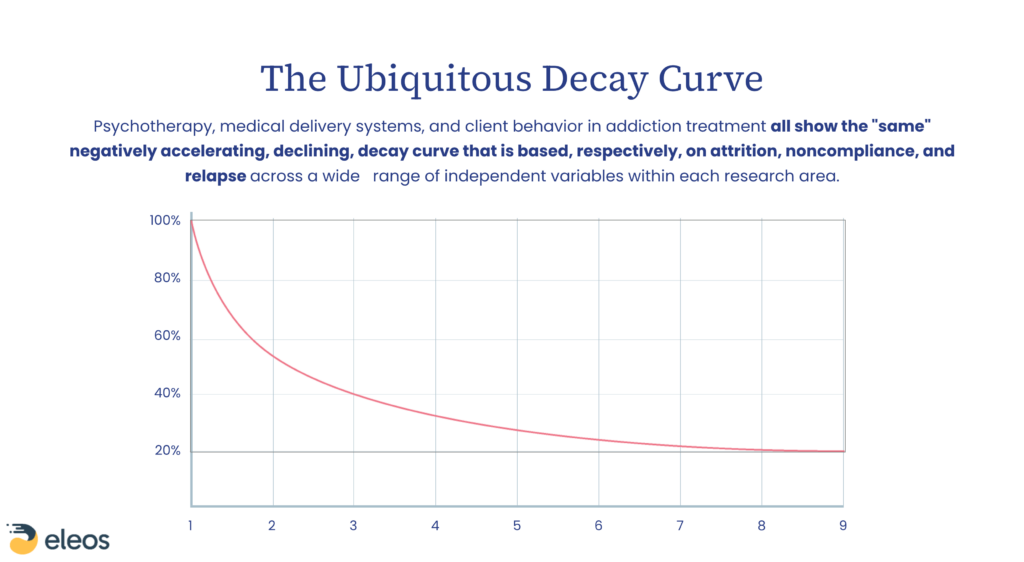
The “ubiquitous decay curve” is real. It appears in every clinical intervention studied, from behavioral health treatment to a 10-day course of penicillin. When you plot retention against sessions over time, the curve is steep, early and almost universal. “You are actually fighting that curve,” Denny said. “If you think of 100% of a population that starts a treatment, every clinical intervention I’ve ever looked at follows a curve like this.”
The research on single-session therapy adds another layer. About 20% of people who come in for mental healthcare only need or want one session. The problem isn’t that they leave after one, it’s that we don’t account for that possibility at intake. We assume everyone is staying, so we load them down with documentation designed for a long-term relationship, during a session that’s really more of a first date.
“That first session is for us more than it is for them,” Denny said plainly. “And so, in a way, it’s not surprising to me that people drop out of treatment prematurely, and that the modal number of sessions is only one.”
When clients do leave after that first session—especially when they said they’d come back and then didn’t—they leave with guilt. That guilt creates a new barrier to re-engagement. It’s not just dropout; it’s dropout with consequences.
The Documentation Thread Running Through All of It
The pink elephant in the room is the thread that ties both sides of premature dropout together: documentation. Documentation on the clinical side and the client side. At the end of the day, documentation burden is not a separate problem from dropout. It’s the same problem.
Teams with the highest no-show and premature dropout rates tend to have the most paperwork. Then the snake begins to eat its tail: Staff actually need no-shows to catch up on documentation. To compensate, organizations overbook staff by 3–4 hours a day just to hit productivity numbers, which drives more burnout, which drives more turnover, which drives more vacancies. In an industry where 40% vacancy rates are the rule, you don’t need a loop that drives more vacancies.
“Documentation makes up the top three reasons that staff are leaving organizations,” Scott said. “But documentation is also the primary reason that consumers are leaving your access process after one to two visits, because they’re so buried in documentation that they feel like it’s hopeless.”
One case study made the point with numbers: a team in the Northeast started with 1,624 unique data elements in their intake process. They were told by compliance that none of it could be cut. After a data mapping exercise, they deleted 1,028 of those elements because they were duplicated, outdated, or never tied to an actual rule. “We have never worked with a team and done data mapping that we did not see them make substantial cuts,” Scott said. “And for me, a substantial cut is at least 30%.”
The example from Massachusetts is even more unbelievable: Through a statewide collaboration, providers went from 10,000 forms to 33—in 9 months.
These bloated documentation counts don’t come from a desire to be redundant—it’s the result of compliance teams too burdened to know what old requirements can be deleted to make room for new ones, and form building teams too burdened to realize the same question might appear multiple times.
What Actually Moves the Numbers
When the webinar moved into Q&A, that’s when the practical tips started rolling in.
“Control what you can control.”
Scott Lloyd, President, MTM Consulting
Build forms to the time, not the other way around.
One of Scott’s best pieces of advice: “Don’t let your forms drive the time. Build your forms to the time you want to spend with the client and the time you have to spend with the client.” If your intake is taking 2 hours, the answer isn’t to schedule 2-hour intakes, it’s to cut the intake.
Rethink the first session entirely.
Denny shared a real example from when he ran a community mental health center. Their second-appointment no-show rate was running at 50%. Their outpatient director redesigned the first visit as a 30-minute “shopping” session—staffed by interns, no formal chart opened, focused entirely on: Why are you here, here’s what we can offer, here’s how long it takes, do you want to do this? If yes, second-appointment no-shows dropped to zero. If no, they left with a card that said, “Call us when you’re ready.”
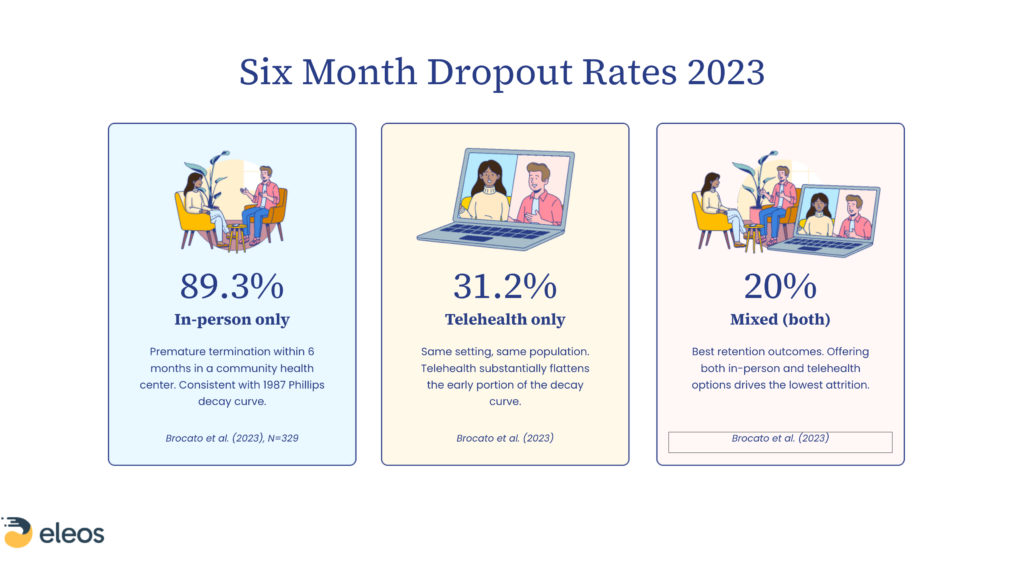
Use a mixed care model.
Research shows that in-person-only treatment has an 89.3% dropout rate within 6 months. Telehealth-only drops that to 31%. A blended model—in-person to build the relationship, with telehealth as a convenience layer—gets it down to 20%.
Treat clients as customers wearing two hats.
In community-based care, we don’t think of our clients as consumers or customers. Because we’re so focused on the care. And clients do come to care as patients, but also as customers, carrying every expectation they’ve ever had from any service industry. If the first session feels like filling out forms that have nothing to do with why they’re there, they’re making a customer decision, not a clinical one. “When they don’t show up for that second session, they’re telling you, ‘I don’t want to buy it.'”
Where Technology Fits In
In healthcare, behavioral or otherwise, it’s very common for staff to hear that technology is going to massively impact their lives, it’s going to make everything better. And so many times, the tech doesn’t live up to the promise. But Denny noted that ambient listening for documentation is different. It’s the first technology Denny has seen that’s actually designed to give time back to the clinician, not just to compliance.
When you pair collaborative documentation practices with AI tools that reduce post-session paperwork—like what Eleos has built—the math changes. “An hour a day, 5 hours a week, 250 hours a year,” Scott said, describing what documentation reduction saves per clinician. That’s time that goes back to care.
The technology, ambient listening or intake assistance, isn’t the magic bullet. It’s a layer that helps once you’ve analyzed the data and identified where you can make a difference. Tech is the accelerant. You have to map your data first. You have to cut what doesn’t belong. Then the AI does more with less—even faster.
The Advocacy Layer
One of the sharpest points of the conversation came from Denny—and it wasn’t about what individual organizations can do. It was about what the industry needs to push for systemically.
Across states, counties, and payers, data collection requirements are often 95%+ redundant. Organizations serving clients across multiple payer systems have to format the same data differently for each one—creating compliance overhead that serves no one, least of all the client. “Getting this on the agenda as something for your trade associations to start dealing with at a kind of systems level” was Denny’s charge to attendees.
Jeremy Attermann from the National Council echoed it: “Now is a good opportunity, I think, in the environment we’re in. The National Council sees some silver linings of opportunities to rethink what is pretty universally seen as burdensome regulations in this early stage of getting someone into care.”
The Stat to Take to Your Next Leadership Meeting
Seventy-five percent of new clients. Gone before the third appointment. This is a system design problem, and client engagement is the symptom, not the disease. But the parts of the system you can change are bigger than most teams realize.
The good news is what Scott said at the top of the session and meant it: “There are things that we can do to move past all of these things, including losing money, or whatever else that we’re seeing.”
Want to see what this can look like inside your organization? Request a demo today.
