






Let’s be honest: The newscycle these days feels like a constant reel of sad, bad, and often, downright chaos.
The headlines swirling in behavioral health and substance use disorder (SUD) treatment are no exception. Since H.R.1 was signed into law on July 4, 2025, the commentary has ranged from urgent to alarmist.
Policy breakdowns. Think pieces. State-by-state speculation. For leaders in the space, the volume of information has been overwhelming, and clear operational guidance has been harder to find.
So here’s the 411. ☎️
On our recent webinar, hosts Dr. Denny Morrison, Chief Clinical Officer at Eleos, and Dominic Miller, LCSW, MPA, Founder and Principal of boutique consulting firm Sotoro LLC and former COO of Southwest Behavioral & Health Services, moved beyond the noise to focus on what matters most for behavioral health and SUD leaders.
Below, we’ve summarized the highlights from their conversation, including:
- What’s actually changing;
- Who will be most affected;
- Where financial pressure will show up; and
- How organizations can prepare now for long-term sustainability.
Want to watch the full webinar? Catch the replay here.
The Basics of H.R.1 and Why It Matters
Unless you’ve been peacefully living under a rock (respectfully 😉), you probably already know that H.R.1—also known as The One Big Beautiful Bill Act (OBBBA)—is a sweeping federal budget reconciliation bill covering tax policy, energy, immigration, and healthcare.
For behavioral health and SUD, the biggest hits include:
- Reductions in federal healthcare spending by approximately $911 billion over the next eight years;
- A 15% drop in federal Medicaid support; and
- Estimates of 10 to 12 million people becoming uninsured by 2034.
With many of these orgs relying heavily on Medicaid reimbursement, the implications of these cuts are significant and long-term.
Why It’s a Double Hit for Community Providers
Community-based behavioral health organizations are likely to feel the impact of H.R.1 even more intensely than other areas of healthcare.
“The pie is shrinking, and it’s not shrinking equally,” said Miller. “The most vulnerable populations are at the [center of the] target.”
These organizations are staring down a perilous one-two punch:
- Because Medicaid funds roughly 25% of behavioral health care in the U.S., a significant portion of previously insured individuals will likely lose coverage.
- Many of those same individuals will still need care—and may return to community-based organizations as uninsured or indigent clients.
This creates a difficult financial dynamic: Reduced reimbursement revenue paired with sustained—or even increased—demand for services.
The Downstream Impact
When individuals lose coverage, the need for care doesn’t go away; it’s often just delayed.
More people will postpone behavioral health or SUD treatment until they’re in crisis, leading to more emergency room visits. And because emergency departments cannot deny care, they’ll absorb costs that could have been prevented upstream.
This is one area where proactive leadership matters.
For community-based organizations, now is the time to ask:
- Which local hospitals and emergency departments can we partner with?
- Is there a coordinated safety net for individuals who can’t access outpatient services due to coverage gaps?
- What do those cross-system conversations look like right now?
Because, as Miller put it, “Hope is not a strategy.”
The Three Core Provisions Driving Medicaid Reductions
Many of the mechanisms included in H.R.1 are not entirely new. As Miller noted, versions of these policies have been tested in the past—often with mixed results.
The nearly $1 trillion (yes, that’s “trillion” with a “T”) reduction in federal healthcare spending is driven by three core mechanisms. Understanding how these provisions work will be essential for planning, budgeting, and operational strategy efforts over the next decade.
Let’s take a closer look at what’s changing—and what these shifts may require from provider organizations.
Tighter Eligibility & More Frequent Redeterminations
Under H.R.1, Medicaid eligibility redeterminations for expansion-age adults will happen every 12 months rather than every 6 months.
The immediate impact is administrative strain: Teams responsible for enrollment and eligibility must manage two redetermination cycles per year instead of one.
For provider organizations, this means:
- Increased eligibility verification workload;
- Greater risk of coverage lapses for clients; and
- Higher administrative costs tied to enrollment support.
Work Requirements
Effective January 1, 2027, Medicaid expansion enrollees ages 19-64 must document 80 hours per month of work, job training, education, or community service.
This provision is projected to account for approximately $326 billion in federal savings—the single largest cost-saving component of the law.
“Having [clients] go through that additional paperwork really falls in the hands of case management staff and frontline workers,” cautioned Miller.
For behavioral health and SUD providers, the operational implications are clear:
- Clients will need support documenting hours;
- Case managers and frontline staff will shoulder additional paperwork; and
- Administrative complexity may increase the risk of coverage loss.
To further complicate things, states are in charge of managing the enforcement of these requirements—leaving plenty of room for ambiguity and inconsistency.
Some states may have robust digital systems and administrative capacity. Others, particularly rural or under-resourced states, may struggle to stand up workable reporting systems—making it even harder for their populations to enroll or be determined eligible for Medicaid.
Limits on State Financing Tools
H.R.1 also restricts states’ ability to use provider taxes and directed payments to draw down federal matching funds.
This provision has received less attention than redeterminations or work requirements. But for many states, it could have more significant consequences.
“This is a quieter provision, but I think it could be potentially devastating for states that have used the tools creatively to fund their behavioral health programs,” explained Miller.
Some states cobble together dollars from these tools to support behavioral health programs that traditional Medicaid reimbursement would not otherwise cover. Restricting these funding options may mean fewer resources flowing back into state systems—even when demand remains high.
Together, these three mechanisms—more frequent redeterminations, increased work requirements, and limits on state financing tools—make up the projected $911 billion in Medicaid spending reductions. Each carries distinct operational implications that require proactive executive planning.
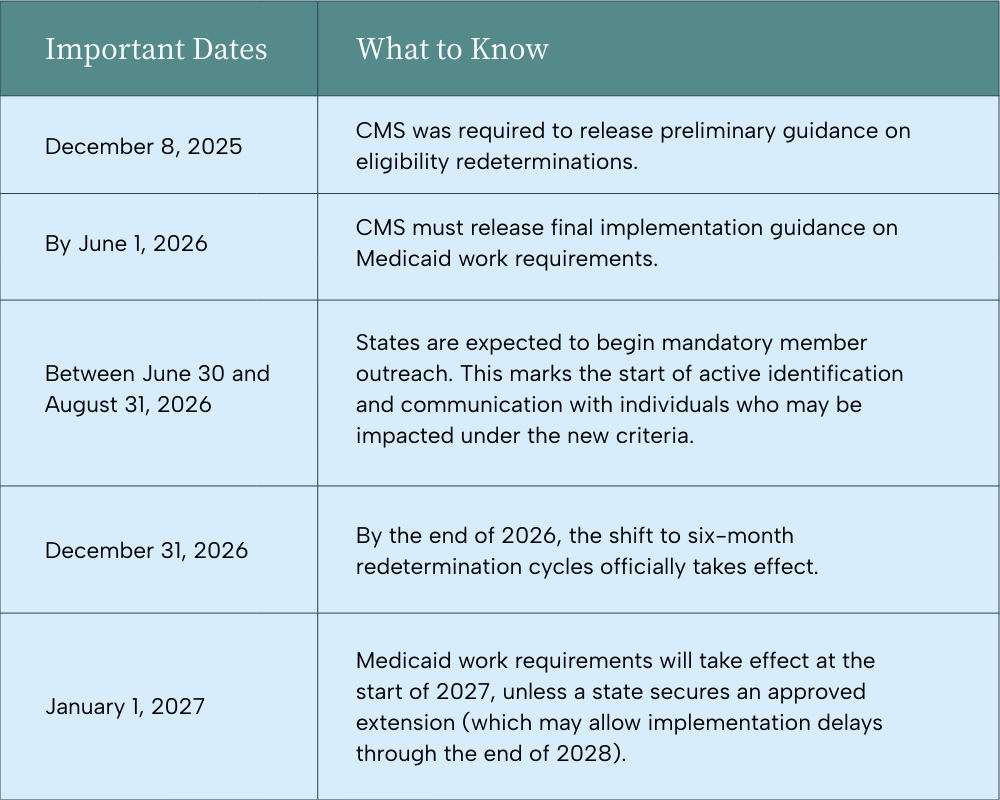
What to Watch and When
Yes, H.R.1 is now law—but enforcement of several H.R.1 provisions hinges on federal guidance and state-level implementation. Still, for behavioral health leaders, understanding the rollout timeline as it currently stands is essential for proactive planning.
Here are the key milestones to monitor:
Exemptions to Eye
The law does include exemptions to work requirements—but definitions will matter.
States are responsible for defining “medical fragility” for their own populations, which in turn determines which individuals are exempt from the new work requirements.
“So, if you’re determined to be medically fragile by whatever that definition is, then with particular work requirements, you’ll be exempt,” explained Miller. “That means enrollees would be exempt from having to go through these extra steps in order to enroll or continue to be enrolled.”
However, as Miller put it, “It’s a double-edged sword.” Because the language remains broad, allowing states to determine their own definitions creates both flexibility and uncertainty.
Translating Policy into Operations
Policy changes don’t live on paper. Behavioral health and SUD organizations have to start planning for how H.R.1 may affect operations.
Here are the organizational impacts you can expect and guidance on how to respond now.
Loss of Coverage
At its core, this legislation increases the risk of coverage loss—particularly for individuals with complex behavioral health needs.
For organizations, that raises difficult (but necessary) questions like:
- If patients lose access to outpatient services, where will they go?
- Will higher-acuity needs surface in emergency departments?
- How does this risk factor fit into our strategic plan?
Higher Admin Burden
If there is one theme that cuts across every provision, it’s administrative complexity.
Redeterminations. Documentation. Reporting. Work requirement verification. Exemption tracking.
This burden will not fall in one place. Consider how it will affect your:
- Clinical and administrative functions;
- Revenue cycle management; and
- Redetermination policy (and how you support it).
More Complex Payer Mix & Higher Uncompensated Care Risk
As Dr. Morrison pointed out, behavioral health already operates within one of the most complex payer environments in healthcare. H.R.1 may intensify that complexity.
“If there’s not going to be that tried-and-true Medicaid funding coming in, then you’re going to find yourself with more grant funding scenarios or sliding scale payer mixes,” explained Miller.
And then, as fewer clients are covered by Medicaid, the risk of uncompensated care goes up.
“As that number starts climbing, I think chief execs and boards are going to have to make some very difficult decisions about what is the limit of their uncompensated care capacity,” said Dr. Morrison.
Boards and executive teams may need to start asking:
- What is the organization’s uncompensated care capacity?
- At what threshold does sustainability become compromised?
- How does shifting payer mix impact things like payroll and employee benefits?
Financial Pressure on Already-Thin Margins
Behavioral health reimbursement rates have historically trailed medical and surgical services. Many nonprofit organizations operate within a 3–5% margin—often by design.
As Miller described, the culture of margins within nonprofits is to “be good stewards of tax dollars and Medicaid funding, making sure that profits aren’t going overboard.” But, in the wake of H.R.1, nonprofit organizations may want to think twice about staying within that 5% margin.
“Margin equals the ability for behavioral health organizations to sustain,” said Miller.
Extra margin is where you can innovate and adapt new technologies that improve efficiency for your clinical staff—so they have more time to focus on the part that matters most: providing care.
Workforce Strain
We’ve heard it time and time again: The demand for mental health services continues to rise, while the pool of clinicians available to provide care continues to shrink. It’s an endless cycle of burnout and turnover that the industry won’t break out of anytime soon.
Especially when H.R.1 layers in additional administrative requirements.
To support their already-stretched workforce, leadership teams should be asking:
- Where can administrative burden be reduced?
- What tasks can be automated or supported with technology?
- How can clinicians be protected from non-clinical task overload?
Elevated Risk for Rural Providers
For rural providers, these challenges are nothing new. But unfortunately, it may get even harder than it already is.
With higher Medicaid dependency, fewer payer options, smaller workforce pools, and greater reliance on local hospitals, rural communities will feel H.R.1 in more significant ways.
That said, there is some good news in all of the doom and gloom. Many of the major provisions will phase in over time, so leaders can plan for what’s coming.
“You have a window, a critical planning window, and it’s only available if you use it,” Miller emphasized.
Potential Pivots to Ponder
With all of that laid out, you’re probably thinking, now what?
Once you get over our incredibly clever alliteration, start thinking proactively with these four “pivots.”
1. Build “Realistic Readiness”
First, assuming the current H.R.1 deadlines hold, start mapping out your plan.
Even if guidance evolves and implementation shifts, planning as though it will all move forward on schedule creates leverage. Waiting does not.
“There’s nothing barring you from doing some scenario-based projections,” said Miller. “And then figuring out ways to model what this would actually look like in terms of dollars and cents at your organizations.”
Map your exposure in terms of:
- Medicaid mix,
- Service lines,
- Geography,
- Redetermination vulnerability,
- Uncompensated care,
- Access/capacity,
- Workforce (turnover/burnout), and
- Acuity/outcomes.
And if you don’t have internal analyst capacity? An outside perspective—whether a consultant, a trusted peer CEO, or even your EHR vendor—can help you uncover blind spots.
Realistic readiness isn’t about having it all figured out, but being prepared for whatever happens when all the policy shifts go into effect.
2. Rethink Eligibility Workflows
Your enrollment processes were built around a 12-month cycle, but that’s changing.
Moving to six-month redeterminations doubles the operational demands. So, the question becomes, can your current teams absorb that?
Now is the time to figure that out by:
- Re-mapping your eligibility workflows;
- Identifying manual steps that could be automated; and
- Pressure-testing whether current staffing models can support increased volume.
One way to streamline admin workflows and prevent coverage churn? Implement an AI tool like Eleos’ OBBBA scanner to alert your providers of patient eligibility changes.
3. Streamline Care Pathways & Modernize Tech
As administrative burdens go up and coverage and reimbursements go down, time is more valuable than ever.
As Miller put it, “Every hour a clinician spends on admin tasks that could be automated is an hour not spent on client care.”
So, get serious about time studies—and about using technology to automate manual tasks that take up too much staff time.
And that doesn’t necessarily mean bringing in shiny new tools. It’s also about using the tools already at your disposal to remove administrative drag and improve efficiency.
See why Dr. Morrison believes group therapy could be a true efficiency win for not only SUD but other behavioral health settings, too.
4. Don’t Go It Alone
Lastly—and this may seem too warm and fuzzy for some—don’t try to navigate all of this alone.
Warm up your partnerships now. That could mean:
- Strengthening relationships with local hospitals;
- Engaging Medicaid leaders early;
- Showing up to policy conversations with data;
- Exploring shared service models;
- Considering affiliation or MSO arrangements; and
- Having honest merger conversations—even if they don’t result in a merger.
“‘Don’t go it alone’ doesn’t just mean, ‘How do we merge, how do we acquire, how do we affiliate it?’” said Miller. “It also means, ‘Who at your organization is your key intergovernmental person that interfaces with the decision maker in the Medicaid system in your state?’”
In other words, know who’s in the room—and make sure you’re in it, too.
Bring your data. Band together. Leaders already know the system is under strain. What they need are concrete examples of how policy changes will play out in real communities—and credible partners who can help design workable solutions.
Don’t Panic, Pivot
In the wise words of Dominic Miller (or so we think—we’re pretty sure he coined the term when it comes to H.R.1):
“Don’t panic. Pivot.”
Yes, this is a tightening environment—there’s no sugarcoating it. Funding pressure is real. Administrative complexity is increasing. Workforce strain isn’t going away.
But it’s also a forcing event. It’s an opportunity to step back and ask:
- Are we structured for the next decade—or the last one?
- Is our tech stack actually supporting our clinicians?
- Are we protecting margin in a way that protects our mission?
- Are we having honest conversations with our board about what must evolve?
As Dr. Morrison put it, “It’s trite, but the old saying, ‘In every crisis, there’s opportunity,’ is true. But it’s only there if you look for it. It’s only there if you’re ready for it.”
Pivoting doesn’t mean having all the answers. It means acknowledging that you can’t keep doing everything the way you’ve always done it and expect different results.
The organizations that use this moment to rethink, streamline, and collaborate will be better positioned for the decade ahead.
If you’re evaluating how to protect margin, reduce burnout, and make your technology work harder for your teams, we’re here to help. We work with behavioral health and SUD leaders every day who are asking the same questions.
Let’s compare notes and talk through what readiness could look like for you.
